




























PAIN BEHIND KNEE: THE ‘OL WALLET-IN-DOOR SYNDROME
PAIN BEHIND KNEE: THE ‘OL WALLET-IN-DOOR SYNDROME
Author’s Gratitude: Big thanks to Dr. Ed House at New York Chiropractic College for sticking his wallet in the door during every Active Rehab meeting. The vision of him, not saying a word, and doing this, has forever been engrained in my mind.
—
Do you have pain behind knee? (That’s how they said it back in the days when the Native Americans ran around this land.)
You probably have the ‘Ol Wallet-In-Door Syndrome.
“PAIN” BEHIND KNEE IS MOST COMMONLY NOT A “PROBLEM” BEHIND KNEE
Test yourself.
Stand up.

Keep your knees straight and touch your toes.

If doing this provokes pain behind your knee, you have a sciatic nerve problem, either coming from an entrapment along the sciatic nerve’s course or from the spine.
This post is not about sciatic nerve “pain behind knee”. That’s for another time.
Now, sit down.
Bend your knee, bringing your heel as close as you can to your butt cheek. If it’s really painful, you can use your handy dandy friend to help you perform this test. Notice in the below example, her knee flexion range of motion stops with her heel 4 finger-breadths away from her butt cheek.

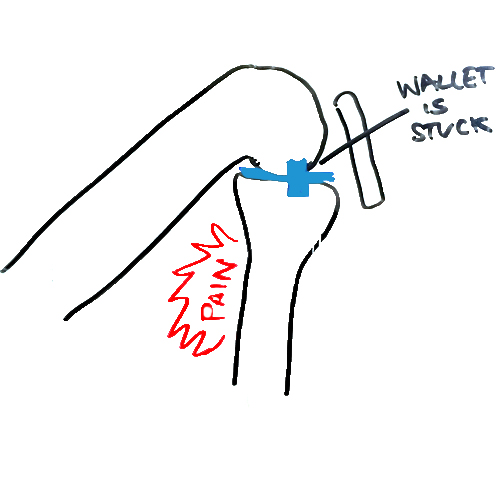
If doing this provokes pain behind your knee, you have a wallet-stuck-in-your-knee-door.
Let me explain.
The wallet is medically speaking, a space-occupying-lesion. It is something that takes up space in the door hinge, not allowing it to fully close.
Most often, the wallet is a meniscus pathology, but it could also be osteoarthritis.
WHAT IS CAUSING THE WALLET IN THE KNEE DOOR HINGE?
As always in reducing pain and restoring range of motion, we have to determine a diagnosis (a name for which problem this is).
You know if your “wallet is stuck” when:
- PAIN: you have pain behind the knee.
- FLEXIBILITY: you cannot bring your heel to your butt (you have restricted knee flexion range of motion).
In the case of the wallet in the knee door hinge, below is a simplified version of the two major issues:
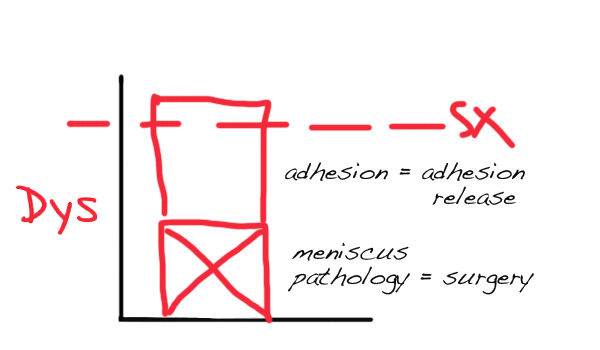
The more significant and more reducible block on our graph is the adhesion.
Removing the adhesion will slow the meniscus pathology’s growth over time.
If the meniscus pathology expresses its symptoms:
… then it may need to be reduced with surgery.
Note: Surgery, in this humble doctor’s experience, never completely resolves meniscus issues. It only makes the block smaller, it doesn’t disappear it.
HOW DO YOU FIX THIS KNEE PROBLEM?
The first place to look for knee adhesion by a practitioner is addressing knee flexion range of motion.
Knee flexion will be restricted, causing pain behind the knee, and creating an excessive amount of tension that can be felt by a skilled practitioner in the:
- knee capsule.
- patellar tendon.
- where the anterior, medial, and lateral meniscus touches the capsule.
- between the LCL and MCL ligaments and the capsule.
This adhesion is present due to overload of the front of the knee. This happened due to ankle and hip restriction and weakness.
Treatment to remove adhesion in the above named structures immediately increases the range of motion and causes permanent, sustainable improvement, even without further treatment.
If the pain goes away temporarily, then comes back, the meniscus pathology (and potential acute inflammation in the joint) is larger than desired. : (
After knee flexion range of motion plateaus in its improvement, adhesion should be explored in the hip and ankles to restore those ranges of motion and increase strength.
 Tell us about your pain behind the knee? Who have you seen? Did it work? How long have you had this problem?
Tell us about your pain behind the knee? Who have you seen? Did it work? How long have you had this problem?
—
If you know of a friend or family member with pain behind knee or restricted knee range of motion, please forward this information to them so they can get the help they need. Fixing your adhesion matters because it improves flexibility, improves function, reduces pain, and restores normal movement to the body so you can enjoy the things you love. Comment below and tell us your story.